
Atma nirbharta. Ayushman Bharat. These phrases carry a lot of firepower behind them for most Indians. Loosely translated they mean “self-reliance” and “long and healthy life for India”. They were meant to make each Indian puff out his chest with pride and hope. But both depend on healthcare.
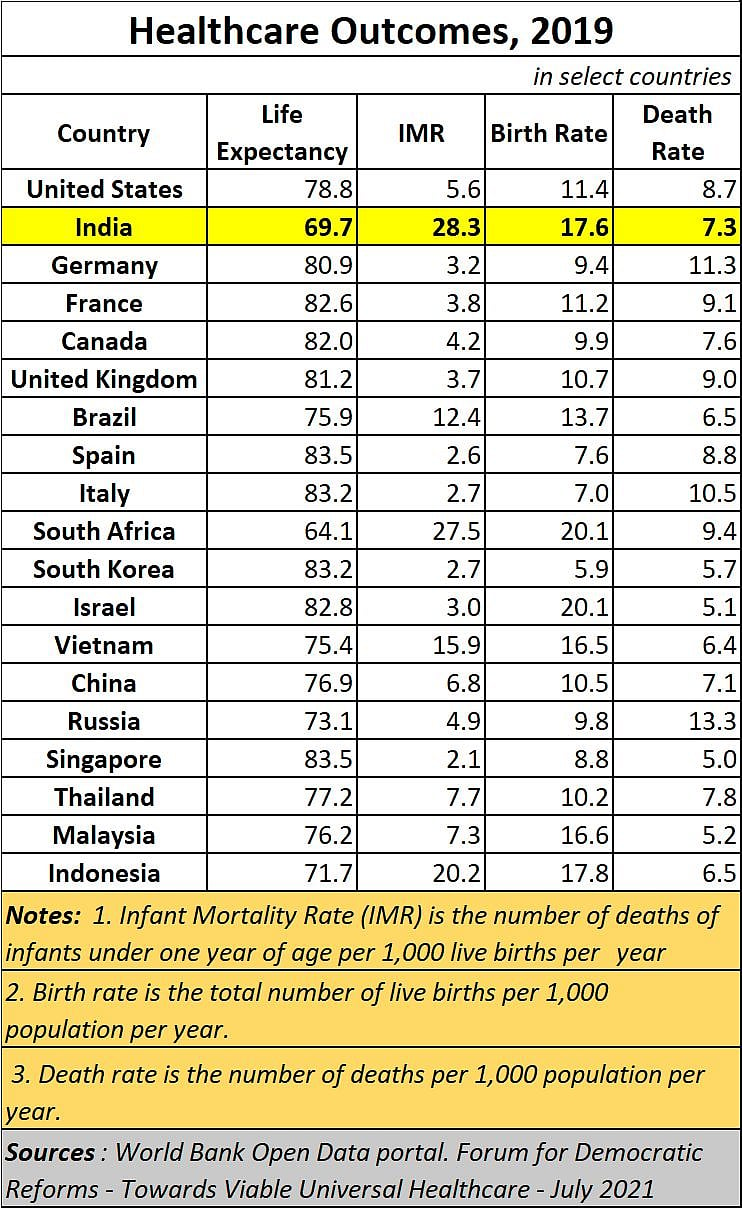
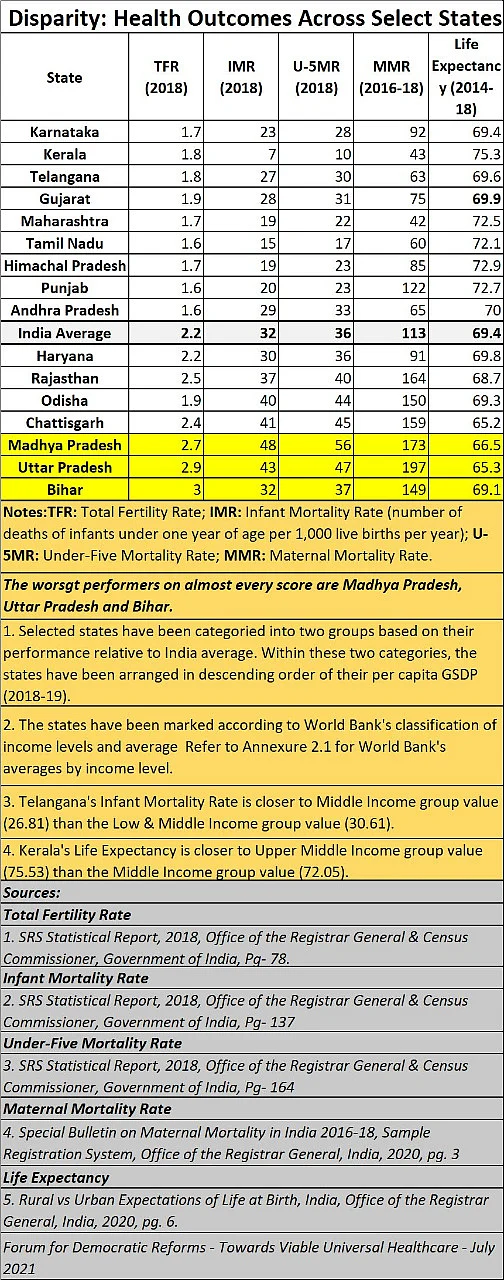
However, slogans are not reality. The fact is that India still has an infant mortality rate of 32 per 1,000. Its maternal mortality death rate is 113 and its average life expectancy is just 69.4 years.
Ailing India
When compared to some global indicators, India’s life expectancy is just above that of South Africa’s 64.
And the worst performing states -- in respect of all parameters covered here – are Uttar Pradesh, Bihar, and Madhya Pradesh. The numbers provide a sharp contrast to the posturing by demagogues who claim that these states have excellent governance standards.
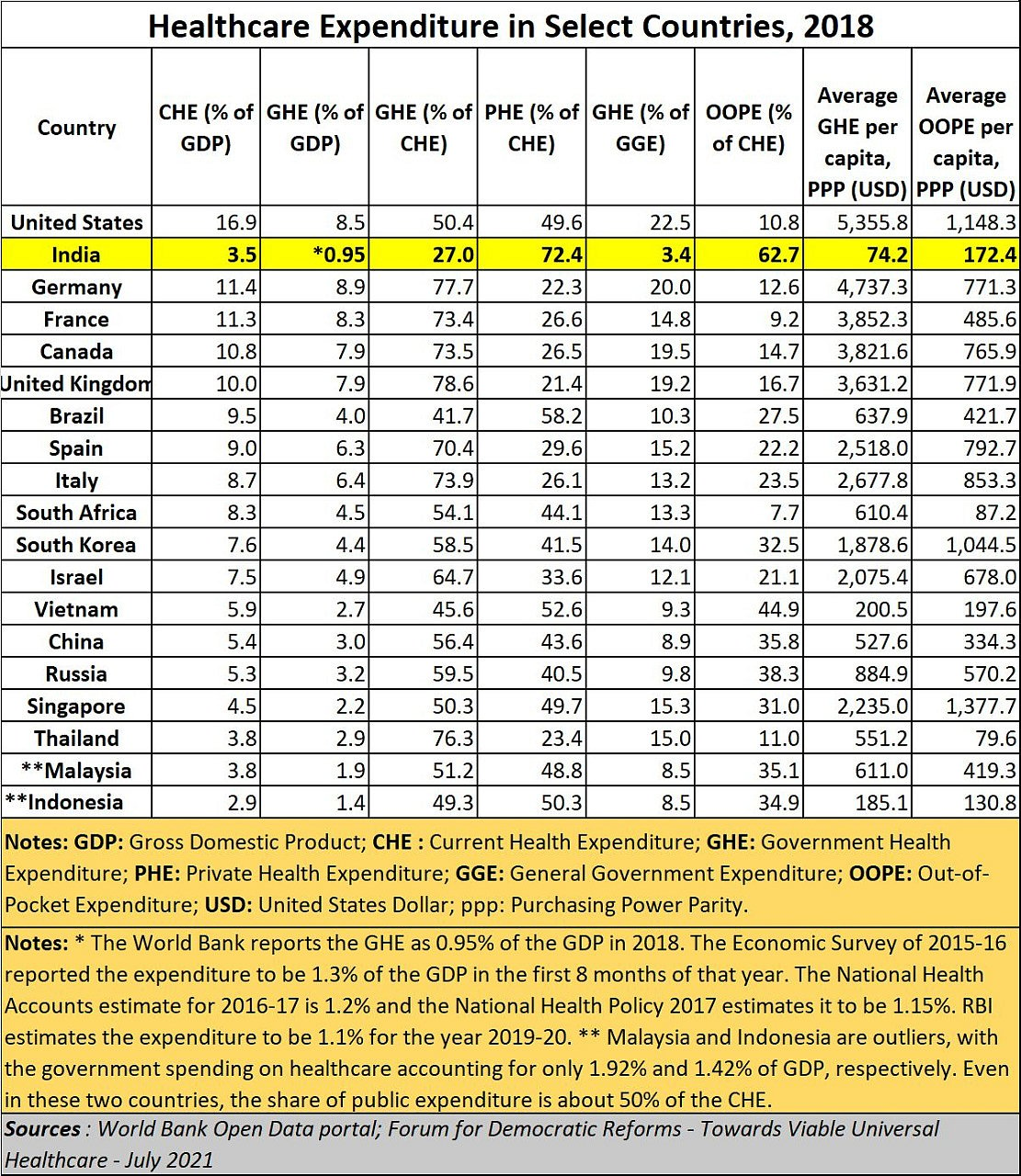
All the data that appears in this article owes much to an excellent report on healthcare, published by the Forum of Democratic Reforms (Towards Viable Universal Healthcare - July 2021- (http://news.loksatta.org/2021/11/launch-of-fdrs-publication-towards.html). This 183-page book replete with over 200 tables and charts, provides many more details about how wanting India’s healthcare systems are.
The tables explain, for instance, how the India’s outcomes are terribly poor when compared to those for other countries.
Clearly, the government – and this refers to successive governments, not just the one in power today – has lost the plot. In repeated attempts to appease the masses, it opted to promote policies of doles and subsidies. Now, it cannot withdraw them. And it thus cannot find the money to spend on healthcare and education. Unfortunately, those two are the building blocks on which economic growth and atma nirbharta rest (https://asiaconverge.com/2020/05/atma-nirbhar-bharat-and-healthcare-headed-for-the-icu/). Without these two, aspirations of becoming a global player become a chimera.
A solution for healthcare
So, what can the government do? Legally, the government is required to provide for quality healthcare (https://asiaconverge.com/2020/06/blighted-vision-for-healthcare-medical-education/) and education (https://asiaconverge.com/2020/08/the-national-education-policy-has-little-vision-less-strategy/) to the masses.
Both are in the dumps. But there is a helpful solution for healthcare – if only the government has the political will and the sagacity.
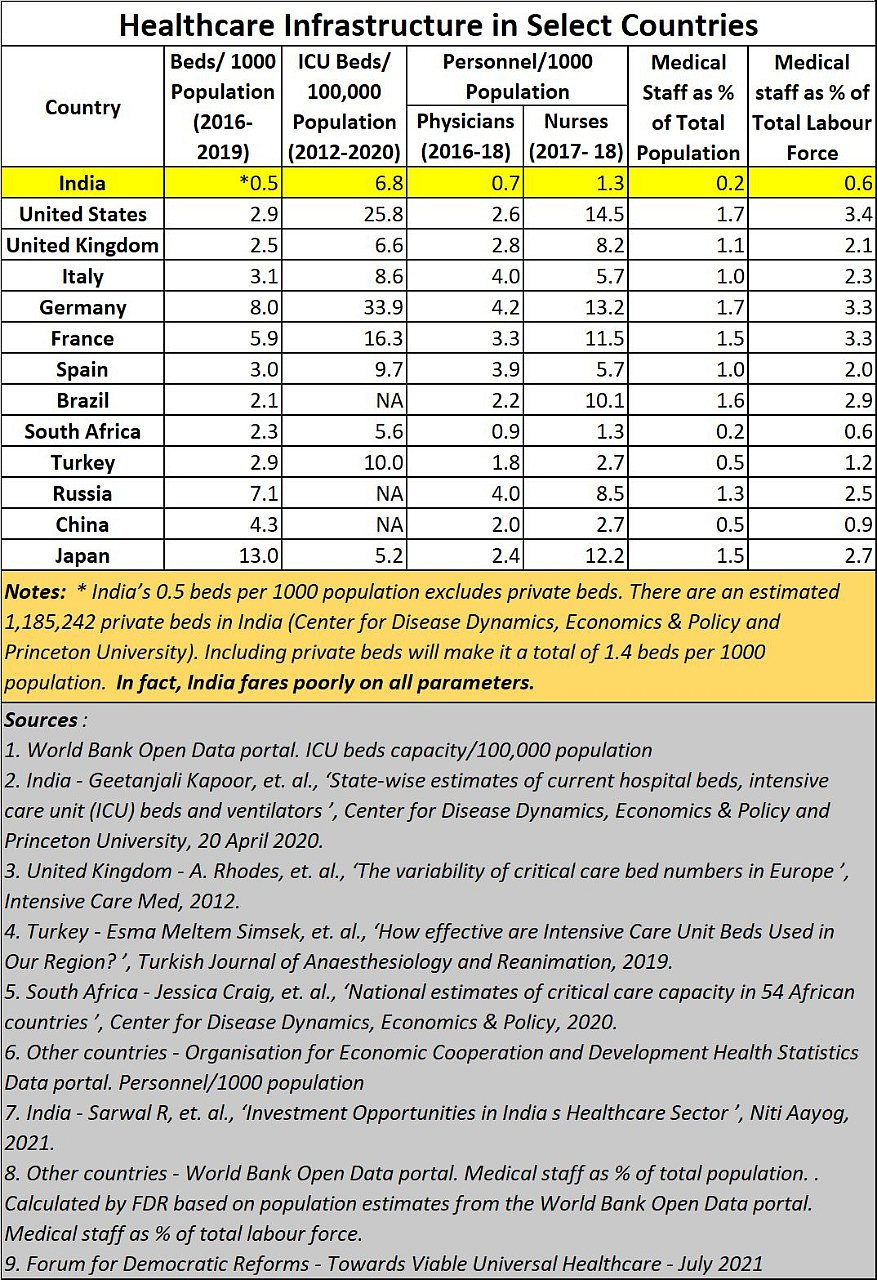
Unlike education, healthcare costs a lot of money. It needs doctors, nurses, hospital beds and plenty of other supporting infrastructure as well. It is common knowledge that India has very few doctors, and few medical colleges. To enhance these numbers India needs much more money.
But for that it must reshape almost all its policies of doles and subsidies. That is politically undesirable. So, it must find another way out.
This is where the government could do something different. It could make the Insurance Regulatory and Development Authority of India (IRDAI) the nodal authority for all matters relating to healthcare (https://asiaconverge.com/2020/06/blighted-vision-for-healthcare-medical-education/).
It will not be easy. But it might be the best way to revamp the entire healthcare sector almost entirely.
Why IRDAI?
But why should IRDAI succeed where the government itself has failed? There are three reasons for this.
First, when it comes to managing any business, the government’s role can be disastrous. Look at the way it is managing the Food Corporation of India (FCI), one of the key reasons why no agricultural laws can work (https://asiaconverge.com/2021/09/need-sensible-laws-to-stop-farmer-exploitation/). That was a major contributing factor to the three agricultural laws being finally withdrawn (https://www.freepressjournal.in/india/large-number-of-farmers-to-gather-at-protest-sites-on-nov-26-says-skm-future-course-of-action-to-be-decided-on-sunday).
Second, the government has announced a grand (grandiose???) scheme under Aayushman Bharat. Like many political announcements in India, it is full of vision (https://asiaconverge.com/2018/08/ayushman-bharat-great-concept-doctors-overlooked/) which have little to do with ground realities.
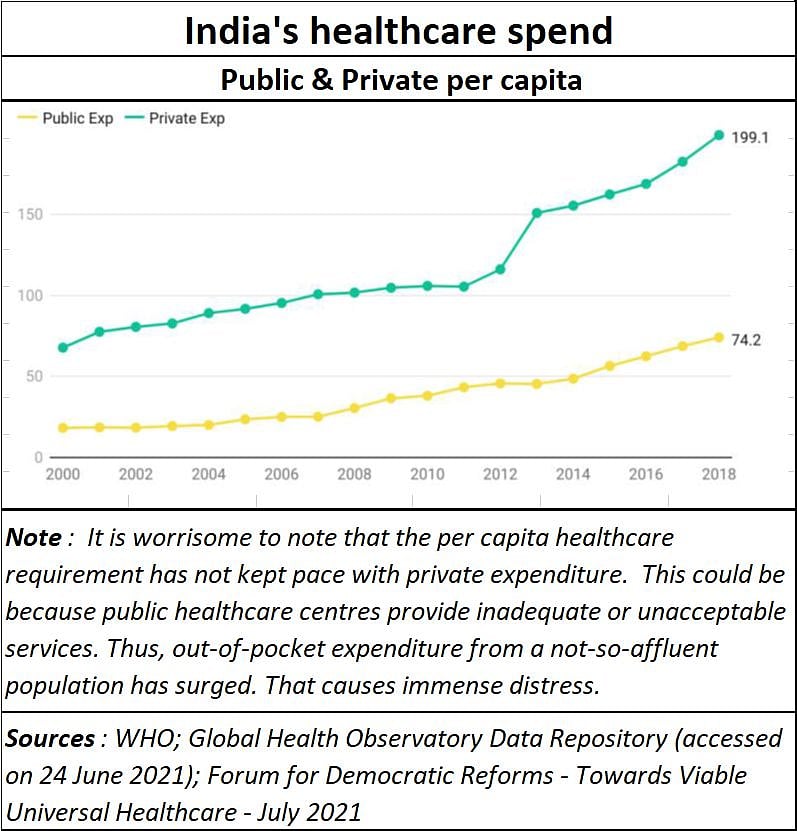
Yes, there is a need for good medicare. And true, there is a need for effective health insurance programme which can reduce the money that individuals have to spend from their own pocket. As everyone knows, it just takes one major ailment to bankrupt a middle-class family because of medical costs. This is what happened to many families when it came to Covid a few months ago (https://asiaconverge.com/2021/04/covid-19-killing-fields-in-india/). The terrible outcomes of poor healthcare management are there for everyone to see. India remains a country with the highest infant mortality cases, and one of the lowest life expectancies.
But the young age of India’s population can be turned into an advantage in getting them to insure themselves at an age when healthcare risks are fewer and manageable. That is where insurance management comes in.
There is another corollary to this.
There must be a way to prevent diseases from taking place. The better the prevention, the lower the health risks, and hence the lower the claims for healthcare costs.
But such preventive measures can only be made possible if pathology, diagnostics and monitoring through networks come under one roof. That is again where the role of the insurance regulator could be of immense significance.
There is a third, and equally compelling, reason for suggesting that IRDAI be transformed into a super regulator for the healthcare sector. Few organisations understand money and risk management as does the insurance sector.
Putting the pieces together
If the role of the IRDAI is structured well, it could actually help channel investments into hospitals and link them up with medical colleges and pathology centres. It could harness all these in such a way that cross subsidisation could take a significant burden off the government’s back. This way, the patients, hence all Indians, benefit. The government benefits too. The healthcare ecosystem and the insurance sector become more vibrant. And India becomes a big hub for healthcare.
India already has excellent private players in place. Some of them have partnered with blue-blooded insurance companies overseas who are known to have very deep pockets and with decades of experience. Health insurance has already been privatised, and the government owned health insurance companies are now being prodded to get themselves listed and break away from government control.
The first priority for the newly formed body will be to increase the number doctors and nurses in India. Without this there can be no meaningful healthcare. If the government is keen on promoting Ayurveda, let it do so the way the Chinese do.
There are hundreds of TCM (Traditional Chinese Medicine) hospitals across the entire country which focus on remedies along traditional lines. The allopathic hospitals are a different stream altogether. India should also do this to prevent dilution and degradation of standards peculiar to each stream of medicare.
Consider the way we have lost out on this front (https://asiaconverge.com/2020/05/education-enriching-other-countries-pauperising-india/). Today, almost 25,000 Indian students study medicine in China. An equal number study the subject in the former Soviet-bloc countries. Even Bangladesh offers admission to some 500 Indian students each year.
India has a big advantage that both China and Bangladesh have. It has hundreds of thousands of patients queuing up for treatment outside almost any government hospital. Medical colleges can function well only if there are patients that students can attend to daily. This is not easily possible in many countries, including the old Soviet bloc territories. The number of patients India can thus be a major advantage.
Quality matters
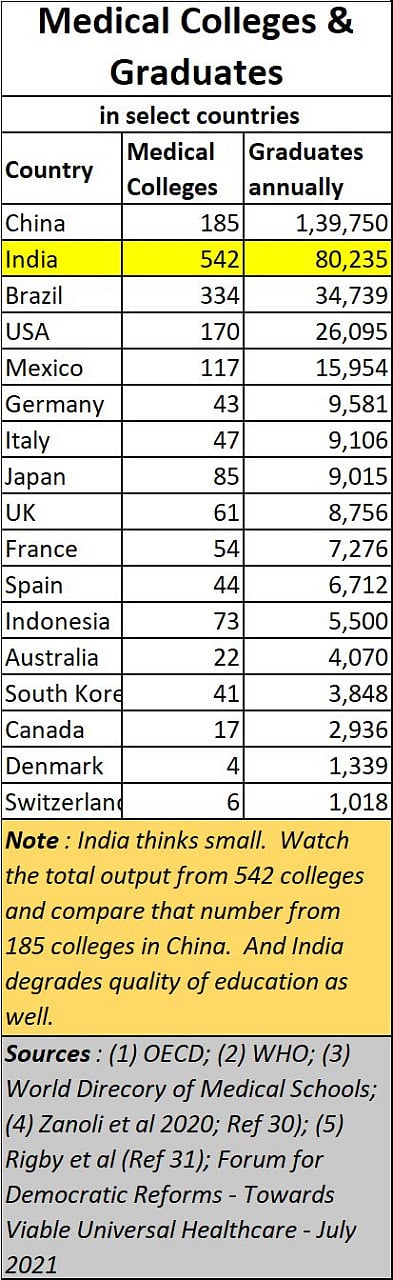
Look at the numbers. China has more graduates coming out of its medical colleges from fewer medical colleges than is the case in India. Most doctors who have interacted with medical students from Chinese centres will tell you that the quality of education in India has been deteriorating rapidly. They will testify to the fact that the quality of education imparted in China is excellent. India has poorer numbers, yet collapsing standards as well.
Quality of education has a lot to do with infrastructure, the quality of teachers, and above all the number of patients a medical student interacts with each day (https://asiaconverge.com/2020/05/atma-nirbhar-bharat-and-healthcare-headed-for-the-icu/). Binding all these together is a good administration that develops systems to monitor each student’s work, and the quality of diagnosis done. Given the politics that medical education has engendered in India, it will not be easy for the government to manage all these.
Ideally, this should therefore be left to the new regulator. He could be authorised, for instance, to allow government hospitals to increase the number of floors of their hospital premises (permission for private hospitals would have to go through the usual channels). Most government owned hospitals are located in prime areas. Each of them has the ability to double – at times even quadruple -- the number of beds, diagnostic centres and even (decent) living quarters for resident doctors, nurses, and other supporting staff.
Financing for these expansions could come through a suitable private public partnership (PPP) arrangement where the private party brings in the funds, in exchange for a certain number of subsidised beds and outpatient treatment facilities. Project approvals and pricing could be left to the newly formed regulator.
Like a hotel has its restaurants, a hospital has its outpatient departments, which engage in diagnostics, and even first aid treatment. They too can be profit centres. Once again, a PPP model could ensure that all those who are insured get their tests at a fraction of the current costs.
Any excuse of a malfunctioning X-ray machine, or an absent pathologist would automatically invite strictures so that government hospitals do not become feeders for private matchbox sized diagnostic centres that can be seen outside such hospitals. The cosy incentives paid to government staff to send patients to these private centres needs to be made a criminal offence immediately.
Benefits
Once the hospitals (with beds and diagnostic facilities) are in place, seats for medical education (for doctors, nurses, and paramedics) could be increased ten-fold within a few years. That would allow India several benefits
Become a centre for medical education for students from all countries. India’s healthcare systems become forex earners.
Reduce forex outgo on students going overseas for medical education.
Provide excellent insurance programmes for all sorts of people. For the poor, the government could channel funds through this regulator, to subsidise the cost of insurance for the needy.
Make Ayushman Bharat a successful programme instead of just a plan on paper (https://asiaconverge.com/2018/08/ayushman-bharat-great-concept-doctors-overlooked/).
Reduce medical expenditure because of preventive care being introduced through careful monitoring and good diagnostics – even through telemedicine networks.
Create enough doctors to cater to the medical requirements for India.
Surplus doctors and nurses could become part of manpower exports to other parts of the world. Nurses are in great demand, especially in countries with ageing populations.
That will allow India to take the next step towards medical tourism and medical research.
In turn, that would help reduce the out-of-pocket expenditure that often bankrupts Indian families when confronted with a major illness at home.
But the way to do this is by putting all controls in the hands of an agency that understands medicare and finance. That is where the healthcare insurance regulator becomes extremely relevant.
The author is consulting editor with FPJ